Incorporating the 2023 ASA Practice Guidelines for Monitoring and Antagonism of Neuromuscular Blockade into our Practice
Earlier this year, the ASA Guidelines for Monitoring and Antagonism of Neuromuscular Blockade were published in Anesthesiology.[1] The Guidelines contain eight recommendations as listed in Table 1.
Table 1
| Recommendations |
1 | When neuromuscular blocking drugs are administered, avoid using only clinical assessment to eliminate residual neuromuscular blockade because the assessment in insensitive |
2 | Quantitative monitoring is recommended over qualitative monitoring to avoid residual neuromuscular blockade |
3 | When using quantitative monitoring, confirm a train-of-four ratio ≥ 0.9 before extubation. |
4 | Use the adductor pollicis muscle for monitoring depth of neuromuscular blockade |
5 | Do not use the muscles of the eye to monitor depth of neuromuscular blockade |
6 | Use sugammadex, rather than neostigmine, to reverse deep*, moderate*, and shallow* depths of neuromuscular blockade induced by rocuronium or vecuronium to avoid residual neuromuscular blockade |
7 | Neostigmine is a reasonable alternative to sugammadex to reverse minimal* depths of neuromuscular blockade |
8 | To avoid residual neuromuscular blockade when atracurium or cisatracurium are administered and qualitative assessment is used, antagonism with neostigmine should be attempted on there is a minimal* degree of neuromuscular blockade. In the absence of quantitative monitoring, at least 10 minutes should elapse from antagonism to extubation. When quantitative monitoring is utilized, extubation can be done once a TOFR ≥ 0.9 is confirmed |
*Definition of depths of NMB
Deep: Post-tetanic count is greater than or equal to 1 and TOF count is 0;
Moderate: TOF count is 1 to 3;
Shallow: TOF count is 4 and the TOFR is less than 0.4;
Minimal: TOFR is 0.4 to less than 0.9
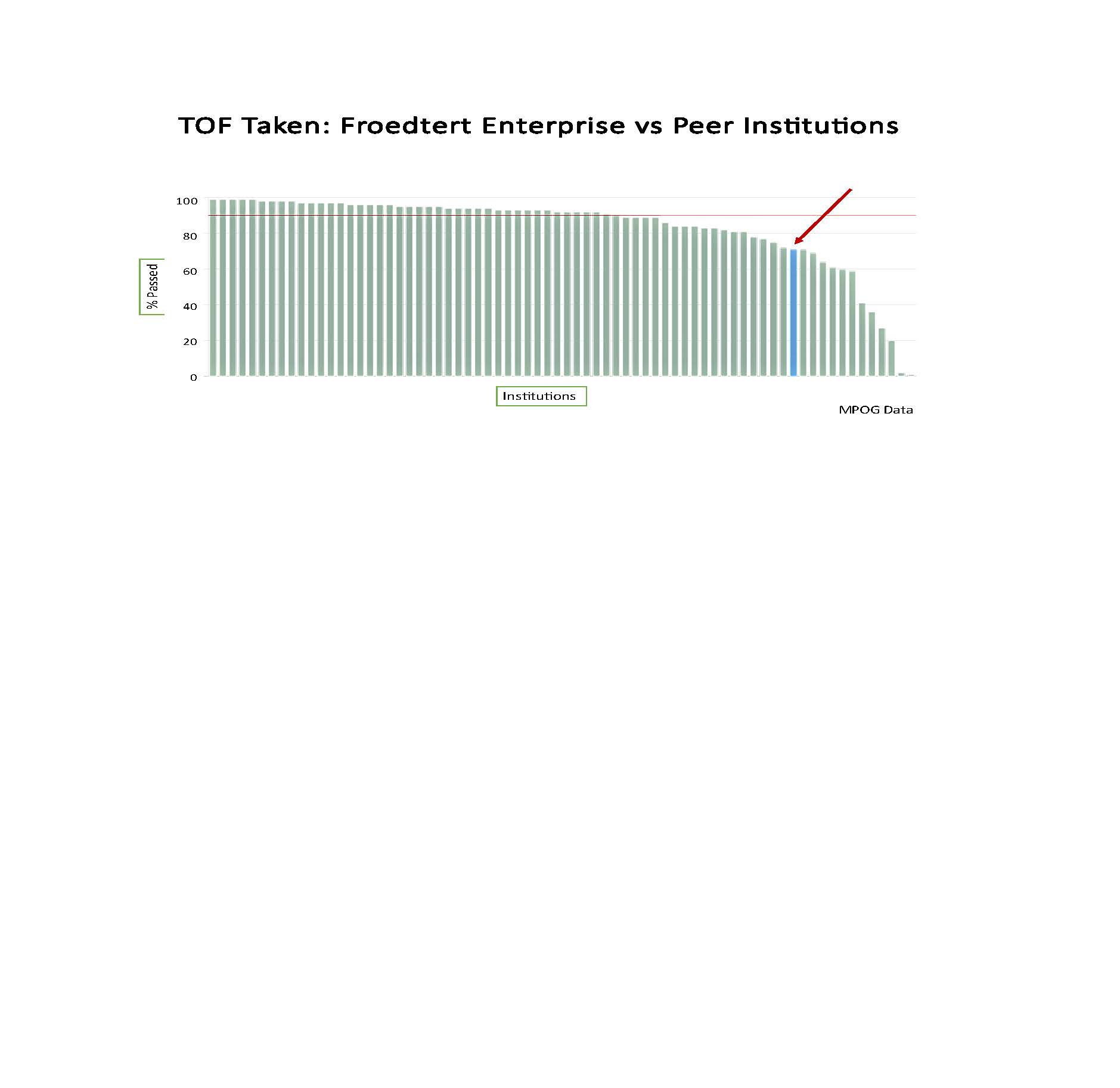
As a Department, our use of quantitative monitors does not compare favorably with that of our peer institutions (see figure 1). Our performance, indicated by the blue line and highlighted by the red arrow is in the bottom 15.
Figure 1
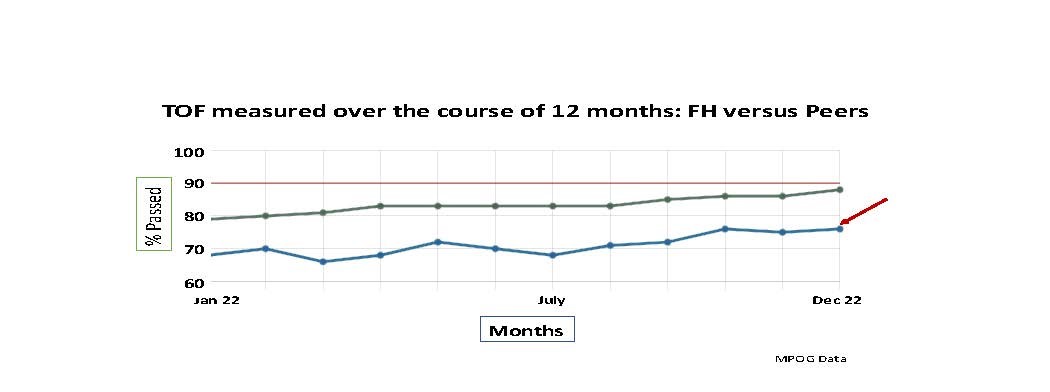
When we look at trends over the 12 months of the previous year, it is apparent that we began with a lower percentage of our patients being monitored and, while use of our monitors has increased, we continue to lag behind the average of our peer institutions (Figure 2).
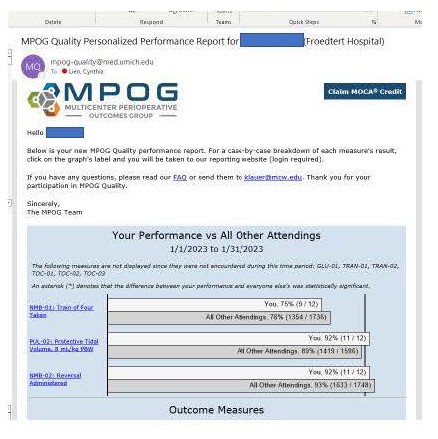
Each faculty member, APP and resident receives their individualized report on monitoring depth of neuromuscular blockade. The reports look like this:
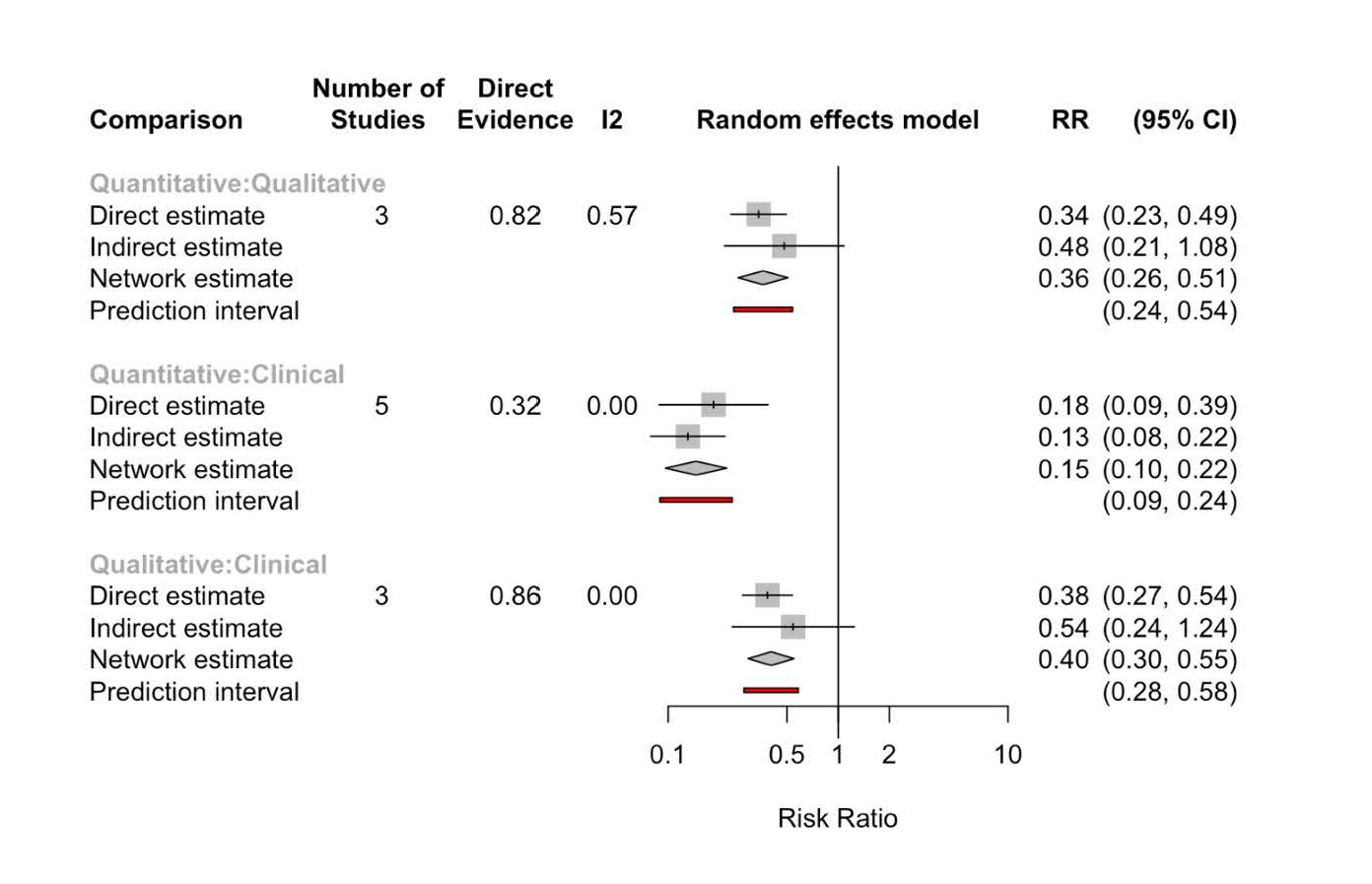
Monitoring depth of neuromuscular blockade decreases the risk ratio of residual paralysis relative to clinical assessment alone and quantitative monitoring decreases it more than qualitative monitoring (Figure 3)1.
Figure 3
Residual paralysis as associated with clinical signs of weakness, an impaired hypoxic ventilatory response, increased risk of upper airway obstruction, increased risk of aspiration, decreased patient satisfaction, and a prolonged PACU stay. As we continue to improve our delivery of evidence-based medicine, it is incumbent on each of us to quantitatively monitor muscle strength whenever a patient receives a NMBA and to record the results in the patient’s EMR.
We will be continuing to follow this metric in MPOG and will provide increasingly granular data in subsequent newsletters.
[1] Thilen SR, Weigel WA, Todd MM, Dutton RP, Lien CA, Grant SA, Szokol JW, Eriksson LI, Yaster M, Grant MD, Agarkar M. 2023 American Society of Anesthesiologists Practice Guidelines for Monitoring and Antagonism of Neuromuscular Blockade: A Report by the American Society of Anesthesiologists Task Force on Neuromuscular Blockade. Anesthesiology. 2023 Jan;138(1):13-41.